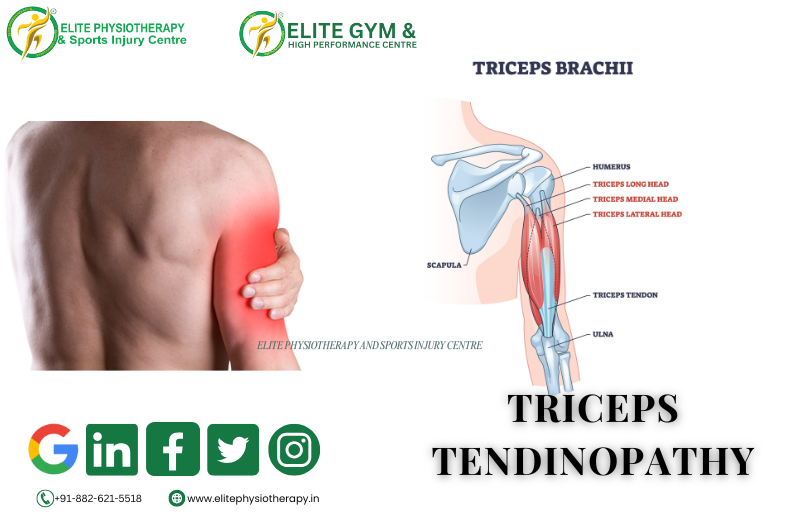
What is Triceps Tendinopathy?
A chronic overuse condition of the triceps tendon, usually around or close to its insertion into the olecranon, is known as triceps tendinopathy. It represents degenerative alterations, collagen disarray, and failed tendon repair rather than acute inflammation. Repetitive microtrauma or overloading the tendon can change its structure, causing discomfort and dysfunction.
Tendinopathy is more degenerative than acute tendonitis, which is inflammatory. Particularly in the early stages, it could coexist with certain inflammatory changes, but in chronic situations, tendon degeneration symptoms are typical.
Causes and Risk Factors
Triceps tendinopathy is predisposed by several factors:
- Weightlifting, throwing, and pushing activities often involve repetitive overload or overuse, which is characterized by repeated extension or resisted loading.
- Microdamage builds up when training volume or intensity is abruptly increased and adaptation time is inadequate.
- Poor technique or biomechanics – inadequate shoulder, elbow, or scapular mechanics that cause the tendon to be loaded asymmetrically.
- Muscle weakness or imbalance: The triceps tendon is subjected to greater strain if stabilizers or synergists are weak.
- Deficits in nutrition and tendon vascularity: Because tendons have a small blood supply, inadequate microcirculation may hinder repair.
- Tendon flexibility decreases with age and degenerative changes.
- Tendon pathology may be exacerbated by comorbidities, which include systemic illnesses such as diabetes, metabolic disorders, or exposure to corticosteroids.
Clinical Features: Signs and Symptoms
When a patient has triceps tendinopathy, they usually exhibit:
- Gradual development of elbow pain in the back, usually proximal or posterior to the olecranon aspect.
- Resisted elbow extension or pushing exercises (such as push-ups or bench presses) exacerbate the pain.
- Palpation of the triceps tendon reveals tenderness, particularly along the tendon or at its insertion.
- Near the end range of elbow flexion or extension, pain may be triggered.
- In more severe cases, a slight grating sensation, known as crepitus, may be present.
- Mild nodules, localized thickening, or swelling of the tendon.
- suppression of triceps contraction due to weakness or pain.
- Potential soreness or stiffness following periods of inactivity (e.g., morning stiffness).
- Decreased functional ability for resistance training or sports in chronic instances.
Physiotherapy Management
Restoring tendon function safely, permitting return to sport, and preventing recurrence are the objectives of an elite sports injury center. Phases can be used to organize the management:
Phase 1: Pain Modulation and Tendon Offloading
- Activity modification/relative rest: refrain from or reduce activities that cause discomfort (e.g., dips, heavy pressing).
- Isometric loading – brief, low-to-moderate-intensity isometric holds—helps maintain tendon homeostasis and lessen pain.
- Cryotherapy, pulsed ultrasonography, and manual soft-tissue treatments (such as tendon massage and cross-friction massage) are modalities for controlling pain and inflammation.
- Stabilization of the shoulder and scapula ensures that proximal mechanics does not overload the distal tendon.
- Mobility exercises include maintaining neighboring joint mobility and gently stretching the triceps (within pain tolerance).
Phase 2: Progressive Loading & Remodeling
- Progressive eccentric loading is the process of gradually increasing load while controlling lowering under resistance.
- Isotonic concentric loading: start concentric strengthening as soon as the pain is tolerated.
- Using heavier, slower loading to encourage tendon adaptation is known as heavy slow resistance (HSR) procedures.
- Integration of sport-specific movement patterns for transfer is known as functional and sport-specific loading.
- Neuromuscular control: avoid compensatory patterns (shoulder shrugging, trunk movement) and concentrate on the quality of movement.
- Soft-tissue mobilization and joint mobilization (of the elbow, shoulder, and thoracic spine) are components of adjunctive manual treatment.
3rd Phase: Return to Sport / High Load & Prevention
- Once the tendon can withstand it, engage in controlled plyometric exercises, such as medicine-ball tosses and explosive push jobs.
- Return to full training load gradually; keep a close eye on symptoms and make small improvements.
- Maintaining and strengthening your muscles can help you develop balanced strength in your triceps, biceps, and shoulder stabilizers.
- Load monitoring and education: make sure you get enough sleep, raise your load gradually, and get technique coaching to prevent recurrence.
- Patient education, load monitoring, frequent reassessment, and progressive growth are essential components of an exceptional center.
Advanced / Adjunct Modalities:
Advanced techniques, including Shock Wave Therapy, Super Inductive System (SIS), High-Intensity Laser, Dry Needling, and Cupping, are available to you at the premium clinic. Here’s how they could be combined.
- Shock Wave Therapy (ESWT / radial / focused)
- In order to promote neovascularization, collagen production, and pain management in chronic tendinopathies, shock wave therapy has been employed.
- Usually, it is saved for instances that have not improved after six or more months of conservative treatment.
- Weekly for three to five sessions, protocols typically use low to moderate intensity, with 2,000 to 2,500 impulses per session.
- Over neurovascular bundles, open wounds, pacemakers, infections, and cancer are among the contraindications.
- For faster healing, Elite Physiotherapy uses loading protocols in conjunction with shock waves that are carefully focused in the tendon region.
- Super Inductive System (SIS)
- SIS, or pulsed electromagnetic induction, is a type of electromagnetic field therapy that is intended to heat tissues deeply and increase cellular activity.
- The idea is to increase vascularity, lessen pain, and stimulate metabolic activity in degenerative tendon tissue, even if there is little high-level data in triceps tendinopathy specifically.
- In practice, loading exercises might be preceded with SIS sessions (e.g., 20-30 min) to increase tissue responsiveness and extensibility.
- High-Intensity Laser Therapy (HILT)
- Class IV high-intensity lasers can speed up tissue repair, lessen discomfort, and promote photobiomodulation.
- Laser therapy may improve collagen remodeling, increase mitochondrial function, and decrease inflammation in tendinopathies.
- Before or after loading workouts, we can administer HILT in cycles (e.g., 2-3 minutes per zone, numerous passes) across the tendon region at the Elite Center, guaranteeing safety and appropriate dosage.
- Dry Needling and Cupping
Why Elite Physiotherapy & Sports Injury Centre Approach Matters
- At Elite Physiotherapy, we adhere to an evidence-based, performance-driven methodology:
- We provide more than simply symptom-based care; we conduct thorough, impartial evaluations.
- Depending on the athlete’s sport, strength, and tendon capacity, we customize loading progressions.
- Instead of depending solely on passive treatments, we mix manual and exercise therapy with cutting-edge modalities (SIS, Shock Wave, Laser).
- In order to prevent flare-ups and guarantee a safe return to sports, we dynamically monitor and modify load.
- Aware of the athlete’s training requirements, we place a strong emphasis on teaching, biomechanics correction, and recurrence avoidance.
- Our patients receive top-notch care that goes above and beyond normal rehabilitation.